1. We do our best work in the dark
2. We can see through your clothes
3. We know all the positions
4. We are well developed
5. The chemistry is always right
6. We know what buttons to push
7. We have all the right techniques
8. We know how to warm up a tube
9. We know how to get the best penetration
10. When you need it now, we make it wet.
Thanks to Kristen from Kristen's Chronicles for the list.
Monday, December 04, 2006
Monday, November 27, 2006
New Rad Links
 Hi Folks! I've recently been alerted to some really useful websites relating to radiography and radiology. Links to these sites are below and have also been added to the side bar.
Hi Folks! I've recently been alerted to some really useful websites relating to radiography and radiology. Links to these sites are below and have also been added to the side bar.Radiology Ramblings
Dave's Places in Radiology
Dave's Radiology Student's Page
Please take a minute to check these sites out. They have tons of useful information for Rad Techs, Rad Tech students and Rad Tech students-to-be!
Wednesday, November 22, 2006
Happy TG
Happy Thanksgiving to everyone! I hope you all have a safe and happy holiday weekend with friends and family. Eat some extra turkey and cranberries for me! :-)
Saturday, November 18, 2006
Office Politics
 Office Politics! Man, I hate that sh!t! Even though we don't work in an office, per se, the politics are there, none the less.
Office Politics! Man, I hate that sh!t! Even though we don't work in an office, per se, the politics are there, none the less.Generally, I try to stay out of office politics. People playing each other off each other, mini vendettas, gossip, grudges; they all seem to get in the way of actually working and doing a good job, but always seem to worm their way in anyway.
Since I've been at clinicals for almost 3 months now at 32 hours per week, people are starting to see me as a coworker rather than a lowly student. So as a consequence, I'm starting to get included in conversations about how so-and-so is a lazy worker and should be fired or how such-and-such is her fault. I prefer to work in a team-oriented atmosphere and I'm starting to realize that that idea might be a little naive, at least at my clinical site.
For the most part everyone puts on a happy face and works efficiently together, if not completely amicably. But once a person leaves the group, they usually start talking about him or her and how they would have done such-and-such differently. I quietly listen and keep my mouth shut. People have a right to vent, but when things get personal thats when I draw the line. I am not there to bad mouth people or talk about how the director sucks, I am there to learn and be taught so I stay as far away from the gossip circle as possible.
The thing that really bothers me is that they usually talk bad about a person who is just having a bad day or even someone who has screwed up just once and had to repeat an exam. So that starts me thinking, "My god, I repeat stuff all the time. What must they say about me, the idiot newbie student." But at the same time I tell myself "Hey I'm allowed to screw up from time to time. Thats why I'm here, to learn. Even if that means learning from my mistakes." So in short, I try not to include myself when the group starts gossiping, and just hope that whatever goes around about me is minimal in its personal attacks on my character. What else can I do, right?
Sunday, November 12, 2006
Tuesday, October 31, 2006
Café
If you're a coffee-aholic like I am, these cartoons will brighten your day. If not, you still might like 'em! :-)
Coffee Cartoons
Coffee Cartoons
Thursday, October 19, 2006
Change of Color
The fall colors are just about at their peak right now in Flagstaff and the city and mountain are gorgeous.
Because of our local climate (i.e. high elevation and very little precipitation), there are very few deciduous type trees that thrive here. Pondarosa pine is the most common type of tree, but the next most common is the aspen.
I love aspens. Not only are they very aesthetically pleasing (at least in my opinion), they also make a wonderful quaking sound when the wind rustles the leaves. Hence the name "quaking aspen", I guess. In the fall, the green leaves turn to a bright yellow color that, as the fall light filters through them, fills the forest floor with a warm, buttery light that keeps you warm even when the air is cool.
Unfortunately it won't be long until the wind and snows come, knocking the foliage to the forest floor. Luckily, we took a hike last weekend and were able to get some great pictures of the leaves. So I'll shut up now and post some pretty pictures. I hope you enjoy them.










Because of our local climate (i.e. high elevation and very little precipitation), there are very few deciduous type trees that thrive here. Pondarosa pine is the most common type of tree, but the next most common is the aspen.
I love aspens. Not only are they very aesthetically pleasing (at least in my opinion), they also make a wonderful quaking sound when the wind rustles the leaves. Hence the name "quaking aspen", I guess. In the fall, the green leaves turn to a bright yellow color that, as the fall light filters through them, fills the forest floor with a warm, buttery light that keeps you warm even when the air is cool.
Unfortunately it won't be long until the wind and snows come, knocking the foliage to the forest floor. Luckily, we took a hike last weekend and were able to get some great pictures of the leaves. So I'll shut up now and post some pretty pictures. I hope you enjoy them.










Saturday, October 14, 2006
Wet Roads, Traumas Arrive
I saw and participated in one of my first major traumas today. It was not a very uplifting experience.
The hospital I'm at for my clinicals is pretty small and most major traumas are automatically sent to Flagstaff or Phoenix since both cities have hospitals that are rated Trauma 1. But today they sent us one for reasons unknown to me.
It was an 18 year old man who had been in an MVA. The poor kid had hydroplaned on some wet asphalt slid off the road and was ejected from the car. He had head, neck and abdominal trauma and was in pretty bad shape. They called us for a stat portable chest and pelvis x-ray and would later do a CT scan of the head and neck areas.
It was amazing to watch the docs and nurses swarm around him, all of them doing their jobs with infinite efficiency. I attempted to do my part, namely x-raying the patient's chest and pelvis, in as timely manner as possible.
Upon visual inspection it was clear the kid was in pretty bad shape and once we got the CT scan there was no denying his condition. The head trauma he had sustained had caused a massive bleed in his brain and he was more than likely brain dead already.
At this point they transfered him to Flagstaff since my hospital doesn't have a very advanced neurology dept. The news of his condition hit me harder than I would have expected. I thought about how his family's life would be forever changed by the events of that day. I did my best to continue on during the day, x-raying patients and keeping a cheery demeanor with them. But I kept thinking about when the doctor would finally have to break the news to the kid's family that he was almost certainly brain dead and would most likely not survive for many more hours. How would I react if I were given the same news about my brother, mother or wife? There is no way to know how one will react until one is put into that situation and with any luck I will never have to find out how I would respond.
The hospital I'm at for my clinicals is pretty small and most major traumas are automatically sent to Flagstaff or Phoenix since both cities have hospitals that are rated Trauma 1. But today they sent us one for reasons unknown to me.
It was an 18 year old man who had been in an MVA. The poor kid had hydroplaned on some wet asphalt slid off the road and was ejected from the car. He had head, neck and abdominal trauma and was in pretty bad shape. They called us for a stat portable chest and pelvis x-ray and would later do a CT scan of the head and neck areas.
It was amazing to watch the docs and nurses swarm around him, all of them doing their jobs with infinite efficiency. I attempted to do my part, namely x-raying the patient's chest and pelvis, in as timely manner as possible.
Upon visual inspection it was clear the kid was in pretty bad shape and once we got the CT scan there was no denying his condition. The head trauma he had sustained had caused a massive bleed in his brain and he was more than likely brain dead already.
At this point they transfered him to Flagstaff since my hospital doesn't have a very advanced neurology dept. The news of his condition hit me harder than I would have expected. I thought about how his family's life would be forever changed by the events of that day. I did my best to continue on during the day, x-raying patients and keeping a cheery demeanor with them. But I kept thinking about when the doctor would finally have to break the news to the kid's family that he was almost certainly brain dead and would most likely not survive for many more hours. How would I react if I were given the same news about my brother, mother or wife? There is no way to know how one will react until one is put into that situation and with any luck I will never have to find out how I would respond.
Friday, October 06, 2006
My First "Tipping" Experience

I had an interesting first experience today. One that most people will never get the opportunity to experience in their lives. I "tipped" a BE patient for the first time.
"Tipping" a patient is a nice way of saying that I inserted the tip of an enema tube into the patient's rectum and administered liquid barium sulfate into their colon. Nice huh?! I hope most of you never have to experience it.
And believe it or not the "tipping" part isn't the worst of it. In many patients the barium, and air that is added later, expands the colon and makes the patient feel like they are having horrible gas cramps. I have never had one myself, but from what the patients have been describing to me during the exam, I hope to never have to have one........or at least put off having one for many years!
BEs are often done in conjuction with or instead of a colonoscopy to look for problems in the large intestine like colon cancer, diverticula, polyps, ulcerative colitis, Crohn's disease or even appendicitis. Most of your organs are not visible on standard x-rays, so in order to visualize the colon a radiopaque material (in this case barium sulfate) is used to coat the inner lining of the large intestine and then air is injected to expand the walls so all parts of the intestine are visible on the x-ray image or under fluoro examination.
BEs are a very common exam and provide the doctors with a lot of good information about the condition of the colon.
Truthfully, I had been dreading my first experience tipping a BE patient. In school the instructors always tell horror stories about techs being pooped on by elderly patients who have not been prepped properly or of patients being unable to hold in the barium and letting loose all over the table. But so far I have not seen this and, although I am sure it happens, I don't think these problems are very common.
I guess I was most concerned with the rather intimate aspect of actually tipping the patient for the first time, but everything went well in this case. I explained to her what I was going to do and made sure she was ready before I did anything. Another tech was there to make sure I did everything correctly.
I'm actually extremely relieved that my first time is over and that it went so well. I know that they wont all go so well, but at least I can always look back and remember that my first BE tipping went smoothly.
Wednesday, October 04, 2006
Tuesday, October 03, 2006
HIV positive patient
I had my first HIV positive patient today. It was a little surreal. She didn't fit any of the stereotypes of what one might have for an HIV positive person. She was young, healthy-looking, well-spoken and polite. She seemed like your typical college-age women from anywhere in the US. She wasn't the one to tell us she was HIV positive (it was evident in her chart) and we didn't talk about it with her. All she needed done was a simple abdominal series and single view chest x-ray, so discussion of her condition was not warranted.
On a lighter note, I did my first shoulder x-ray today. Not too exciting but the pictures sure came out pretty. The shoulder is a really strange and complex joint and it's a wonder more people don't have problems with it. The patient needed both shoulders radiographed (he had been bucked off his horse a few days earlier). The tech I was with did the first one, showing me his techniques for positioning, and I positioned the patient for views of the other shoulder. Unfortunately, I couldn't comp this time because I have to do at least one exam with supervision before I can actually comp on it, but I'll be ready next time.
came out pretty. The shoulder is a really strange and complex joint and it's a wonder more people don't have problems with it. The patient needed both shoulders radiographed (he had been bucked off his horse a few days earlier). The tech I was with did the first one, showing me his techniques for positioning, and I positioned the patient for views of the other shoulder. Unfortunately, I couldn't comp this time because I have to do at least one exam with supervision before I can actually comp on it, but I'll be ready next time.
On a lighter note, I did my first shoulder x-ray today. Not too exciting but the pictures sure
 came out pretty. The shoulder is a really strange and complex joint and it's a wonder more people don't have problems with it. The patient needed both shoulders radiographed (he had been bucked off his horse a few days earlier). The tech I was with did the first one, showing me his techniques for positioning, and I positioned the patient for views of the other shoulder. Unfortunately, I couldn't comp this time because I have to do at least one exam with supervision before I can actually comp on it, but I'll be ready next time.
came out pretty. The shoulder is a really strange and complex joint and it's a wonder more people don't have problems with it. The patient needed both shoulders radiographed (he had been bucked off his horse a few days earlier). The tech I was with did the first one, showing me his techniques for positioning, and I positioned the patient for views of the other shoulder. Unfortunately, I couldn't comp this time because I have to do at least one exam with supervision before I can actually comp on it, but I'll be ready next time.
Camping trip to Lockett Meadow
Here are some pics from my wife and my camping trip to Lockett Meadow, a few miles north of Flagstaff, AZ. The meadow and hills are full of aspen and in the fall the colors are amazing. Our campsite is at about 9000 ft asl, so the nights are already pretty cold....... like 25 degrees F cold!! But we brought plenty of blankets and the fire kept us warm until we headed for the sleeping bags. It was so cool to hear the elk bugling in the distance. They kept at it for hours. My wife was sure the male was looking for a booty call! :-) Anyway, enjoy the pics.
 Our camp site
Our camp site
 Becky looking at the San Francisco Peaks from Lockett Meadow
Becky looking at the San Francisco Peaks from Lockett Meadow
 Me at a pulloff on our way to Lockett Meadow
Me at a pulloff on our way to Lockett Meadow
 Becky holding an aspen leaf
Becky holding an aspen leaf
 View from Lockett Meadow the morning after we camped
View from Lockett Meadow the morning after we camped
 Yeah...........it was frickin' cold!!!!!!
Yeah...........it was frickin' cold!!!!!!
 Me contemplating the meaning of life or something just as philosophical, I'm sure ;-)
Me contemplating the meaning of life or something just as philosophical, I'm sure ;-)
 aspen
aspen
 interesting plant
interesting plant
 Becky holding some aspen branches
Becky holding some aspen branches
 Our camp site
Our camp site Becky looking at the San Francisco Peaks from Lockett Meadow
Becky looking at the San Francisco Peaks from Lockett Meadow Me at a pulloff on our way to Lockett Meadow
Me at a pulloff on our way to Lockett Meadow Becky holding an aspen leaf
Becky holding an aspen leaf View from Lockett Meadow the morning after we camped
View from Lockett Meadow the morning after we camped Yeah...........it was frickin' cold!!!!!!
Yeah...........it was frickin' cold!!!!!! Me contemplating the meaning of life or something just as philosophical, I'm sure ;-)
Me contemplating the meaning of life or something just as philosophical, I'm sure ;-) aspen
aspen interesting plant
interesting plant Becky holding some aspen branches
Becky holding some aspen branchesSaturday, September 30, 2006
the Good with the Bad
Working in a hospital is always interesting. You see things you would never see in other jobs. To work there, however, you must take the good with the bad. You are usually seeing people at their worst, most vulnerable point, and you have to be sensitive to that.
In the short time I've been working in the radiology department I have seen some great things, but, unfortunately, some not so great things as well.
For example, on Friday I assisted with an UGI Series on a patient who had been complaining of acid reflux and abdominal pain. During an UGI Series the patient swallows barium and we watch it pass thru their GI tract on fluoro. After we were done and the patient was changing back into their clothes, the doctor pulled me aside and showed me some of the shots he took of her stomach during the exam.
He pointed to a large, rough section of her stomach wall and explained that part of her stomach was being destroyed by cancer and could been seen on the film. Stomach cancer is one of the worst to get and metastasizes very quickly.
It was a strange and sad feeling to stand there and know that this person has cancer and probably doesn't have many more months of life left and she didn't even know it yet. Up until then I hadn't really seen too many major pathologys, just broken bones, diverticula and hiatal hernias, all of which are relatively benign compared to this patient's problem. I'm thankful that I wasn't the one to have to give her the bad news, but I'm also thankful that I was involved in diagnosing her problem, so that she may enjoy the time she has left.
Fortunately, I've also been there when patients have received good news. A couple weeks ago we had another patient in for another Upper GI series but this one also included a small bowel follow thru, where you follow the barium through the small intestine until it has reached the juncture with the large intestine.
In this patient's case, the exam was ordered because his doctor suspected the patient had a bowel obstruction, which is a simple thing in concept but can be very dangerous and life threatening for the patient. He drank the barium and we watched for over an hour (taking pics every 15 min) as it passed through his upper GI and into his small intestine. He had already had a barium enema a few days before so the doc knew that his large intestine was not blocked, so if he was obstructed it would have to be in the small intestine.
But as we watched the barium progress through his system it was clear that there was no obstruction, which meant he would not have to have emergency surgery as the doctor suspected. I still remember the look on his face as the doctor told him the news that he wouldn't have to have surgery. He was so happy and relieved I couldn't help but smile and congradulate him on the good news. It was a good moment for me and I felt lucky I could be there for it.
In the short time I've been working in the radiology department I have seen some great things, but, unfortunately, some not so great things as well.
For example, on Friday I assisted with an UGI Series on a patient who had been complaining of acid reflux and abdominal pain. During an UGI Series the patient swallows barium and we watch it pass thru their GI tract on fluoro. After we were done and the patient was changing back into their clothes, the doctor pulled me aside and showed me some of the shots he took of her stomach during the exam.
He pointed to a large, rough section of her stomach wall and explained that part of her stomach was being destroyed by cancer and could been seen on the film. Stomach cancer is one of the worst to get and metastasizes very quickly.
It was a strange and sad feeling to stand there and know that this person has cancer and probably doesn't have many more months of life left and she didn't even know it yet. Up until then I hadn't really seen too many major pathologys, just broken bones, diverticula and hiatal hernias, all of which are relatively benign compared to this patient's problem. I'm thankful that I wasn't the one to have to give her the bad news, but I'm also thankful that I was involved in diagnosing her problem, so that she may enjoy the time she has left.
Fortunately, I've also been there when patients have received good news. A couple weeks ago we had another patient in for another Upper GI series but this one also included a small bowel follow thru, where you follow the barium through the small intestine until it has reached the juncture with the large intestine.
In this patient's case, the exam was ordered because his doctor suspected the patient had a bowel obstruction, which is a simple thing in concept but can be very dangerous and life threatening for the patient. He drank the barium and we watched for over an hour (taking pics every 15 min) as it passed through his upper GI and into his small intestine. He had already had a barium enema a few days before so the doc knew that his large intestine was not blocked, so if he was obstructed it would have to be in the small intestine.
But as we watched the barium progress through his system it was clear that there was no obstruction, which meant he would not have to have emergency surgery as the doctor suspected. I still remember the look on his face as the doctor told him the news that he wouldn't have to have surgery. He was so happy and relieved I couldn't help but smile and congradulate him on the good news. It was a good moment for me and I felt lucky I could be there for it.
Wednesday, September 27, 2006
List of Stupids
Below is but a short list of things patients have done to land them in our x-ray department.
- drive an ATV drunk......and at night.
- drop a box of frozen french fries on their foot
- jump off a swing
- tried to do a "wicked cool" trick on their skateboard
- slammed their elbow in the refridgerator door
- got out of a car wearing very high heels and turned their ankle
- got a bowel obstruction (OK, so this one isnt so funny)
- wiped out pulling a wheelie on their motorcycle
- hit a light pole while driving drunk (but decided not to come in for two days!!)
- got bumped in their recently operated on elbow by a waitress
- got pneumonia (Again, not so funny)
And my all time favorite...
- they put their leg down in an attempt to stop an 800 lb. ATV going 20 mph instead of using the break.
You would think that the last one would be an isolated incident, but unfortunately it is not. It happens all the time with ATV and motorcycle riders.
So do your best to avoid doing any of the above activities because I'd rather not see YOU at the other end of my x-ray machine any time soon.
- drive an ATV drunk......and at night.
- drop a box of frozen french fries on their foot
- jump off a swing
- tried to do a "wicked cool" trick on their skateboard
- slammed their elbow in the refridgerator door
- got out of a car wearing very high heels and turned their ankle
- got a bowel obstruction (OK, so this one isnt so funny)
- wiped out pulling a wheelie on their motorcycle
- hit a light pole while driving drunk (but decided not to come in for two days!!)
- got bumped in their recently operated on elbow by a waitress
- got pneumonia (Again, not so funny)
And my all time favorite...
- they put their leg down in an attempt to stop an 800 lb. ATV going 20 mph instead of using the break.
You would think that the last one would be an isolated incident, but unfortunately it is not. It happens all the time with ATV and motorcycle riders.
So do your best to avoid doing any of the above activities because I'd rather not see YOU at the other end of my x-ray machine any time soon.
Friday, September 22, 2006
Apologies
 I apologize for the lack of postings the last few weeks. The truth is I'm still pretty exhausted when I get home from clinicals at the end of the day and find it hard to form a complete, coherent thought much less attempt to compose a witty and entertaining post. Not that I have ever been successful at that in the past! :-P
I apologize for the lack of postings the last few weeks. The truth is I'm still pretty exhausted when I get home from clinicals at the end of the day and find it hard to form a complete, coherent thought much less attempt to compose a witty and entertaining post. Not that I have ever been successful at that in the past! :-P Unfortunately, I no longer have the big, healthy doses of spare time I used to have while I was living in Phoenix and only going to classes. I now have to use what little free time I have for doing housework, running errands, spending time with my wife and the all important job of entertaining the cat.
I know, excuses, excuses, excuses. I don't mean to justify my relative absence to the blogosphere, but there are some good reasons I have not been around. I hope my loyal readers will not lose faith in me and go off in search of greener and more frequently updated pastures, and I hope my new readers, especially those of the rad tech student persuasion (you know who you are) will continue to check my site for my not-so-witty, not-so-entertaining updates. ;-)
And now, as I see the spaghetti water is finally boiling, I must bid you all a fond adieu. Enjoy the weekend and please do check back from time-to-time for updates on the life and times of X-ray Tech Student (Formerly) in Phoenix.
Tuesday, September 12, 2006
Poor Little Guy
 "Oowwww!!! Why are you hurting me!!?!?" he screamed in my face. "I'm sorry 'Jimmy'*, I know it hurts. Just be as brave as you can and we'll be done soon, OK?" I replied.
"Oowwww!!! Why are you hurting me!!?!?" he screamed in my face. "I'm sorry 'Jimmy'*, I know it hurts. Just be as brave as you can and we'll be done soon, OK?" I replied.'Jimmy', the poor little guy, had fallen off a swing at the park and broken his wrist. How did I know it was broken? Well, it looked something like this. So, although I'm no doctor, it was pretty safe to say it was broken.
{kind=link}
His parents brought him into the ED about 30 minutes earlier and the doc had ordered a stat 2 view order for his wrist, and with good reason. So I and another tech hurried to the ED to take the x-rays, develope them and get them back to the doc as soon as we could. 'Jimmy's' parents and the other tech positioned his arm, while I got the portable x-ray unit in position. We needed a PA and Lateral view of the wrist, so poor 'Jimmy' had to endure the pain as we switched cassettes in between x-rays.
Being seven isn't easy, but being seven with a severaly broken wrist really isn't easy. But he was brave and put up with our manipulation of his injuried limb with much less protest than I would have thought.
Once back in the rad dept, we developed the images and took a look at them to make sure the density and contrast was right and all pertinent body parts were in view. From looking at the image it was apparent that 'Jimmy" had sustained some major trauma to his wrist. He had broken his distal ulna and radius just below the head, and the bones had displaced and were no longer in line, hence the gruesome look of his arm.
{kind=link}
It was a difficult situation. You're torn between getting a quality image that will give the doctor all the information he needs about the injury, but at the same time you absolutely don't want to cause any more pain to the pt, in this case a child, than is necessary. Overall, the tech did a great job comforting the pt and his parents who were visibly upset. I just hope that with time and "practice" I will be competent enough to do as good a job as this tech did.
*all names have been changed to protect patient privacy.
Saturday, September 09, 2006
Battlefield Radiography
The above is a video produced during the 1940s about a new technology used to treat wounded soldiers on the battlefield. It seems to be similar to a mobile fluoro unit or C-arm that is used today in surgery.
Notice that neither the patient nor the doctors have shielding of any kind and are probably receiving very high doses of radiation. Oh how times have changed.
The above is a video produced during the 1940s about a new technology used to treat wounded soldiers on the battlefield. It seems to be similar to a mobile fluoro unit or C-arm that is used today in surgery.
Notice that neither the patient nor the doctors have shielding of any kind and are probably receiving very high doses of radiation. Oh how times have changed.
Thursday, September 07, 2006
Surgery
 Today I had my first experience in surgery.
Today I had my first experience in surgery.I wasn't in the door two seconds and L grabbed me and we were on our way to assist in surgery. The docs were doing a hip pinning and needed fluoro guidance.
We made our way up to the OR and went into the surgical prep room. L handed me a long white, paper suit, and told me to put it on. "We always have to wear the bunny suit in surgery" she tells me. "Ha ha" I thought, "lets make fun of the newbie student and dress him up all stupid-like." But as I watched she pulled one out for herself and started putting it on. "OK, fine" I thought "I'll put it on if she has one too. How stupid could I look, right?" Well, as it turns out pretty stupid, but at least I wasn't only one.
{kind=link}
After that we made our way to OR Room 3 where the docs had already prepped the pt for a hip pinning. This is where they insert a few metal pins, although bolts is more accurate, into a bone to reinforce it. They needed us, or rather L, to run the fluoro machine so they could correctly position the pins in the pt's hip.
The mobile fluoro machine, more commonly called a C-arm, is a type of x-ray machine that creates real-time images. Instead of producing x-ray "snapshots" like a regular x-ray machine, it uses x-rays and a special sensor to send a live, moving picture of the patient's bones and/or organs to a TV screen. This allows the doc to see precisely where he or she has positioned the pins.
{kind=link}
It was very interesting and I'm looking forward to getting back in there again soon. It's a bit intimidating, however, and I am already dreading the day I screw something up and get chewed out by the surgeon, but I think it will also be an amazing experience.
Wednesday, September 06, 2006
First Two Weeks
 Wow, folks. I really apologize for the relative scarcity of posts lately. Not that there are thousands out there hanging on my every word, but I know some people like to check out this blog on a somewhat regular basis and I hope I don't lose those readers. You know who you are! ;-)
Wow, folks. I really apologize for the relative scarcity of posts lately. Not that there are thousands out there hanging on my every word, but I know some people like to check out this blog on a somewhat regular basis and I hope I don't lose those readers. You know who you are! ;-) Anyway, the past two weeks have been my first two weeks of clinicals in radiography. For those of you who have done clinicals, you know the first few weeks are the most challenging. Everything is new to you, there are about a million things to learn and more is expected of you than you think can be done in a lifetime. But so far I'm surviving and keeping my head above water, well most of it anyway. My chin and mouth sink below the waves from time to time.
At this hospital the Out-patient radiology dept is separate from the in-patient radiology dept. In fact they are on opposite sides of the hospital from each other. I spent my first week in the out-patient dept and was paired up with another rad tech. Let's call her L, for anonymity's sake. The out-patient dept is relatively slow I came to find out, although it didn't seem that way to me at first. In out-patient we do rather routine examinations like chest x-rays and x-rays of the spine, extremities and ribs, as well as mammography and DEXA scans (bone density scans). These are exams that are not emergent, don't require complex equipment or doctors and very little, if any, prep is needed on the part of the patient.
I was able to observe and take part in several exams. My first couple were for the L-spine, the pelvis and hip, the wrist and the foot and lots and lots and lots of chest x-rays. Chest x-rays are so common, in fact, that they have a room entirely dedicated to doing just chest x-rays. Chest x-rays are ordered for anything from shortness of breath (SOB) to pneumonia to suspected fluid in the lung. Luckily this is a fairly simple exam and I have already done several myself, with tech supervision of course. I suspect that a routine chest x-ray will be the first exam I "comp" on. (comp = competency, doing the entire exam successfully myself with no corrections from the supervising tech).
This week was different however, in that I wound up in the in-patient dept.
 Which means a whole new batch of procedures and exams to learn, and learn quickly. Luckily they partnered me up with L again (most of the time) and she is a fantastic teacher. She has only been a tech for 3 years, which helps because she remembers how overwhelming everything can be at first and how much there is to learn and how little time there is to learn it.
Which means a whole new batch of procedures and exams to learn, and learn quickly. Luckily they partnered me up with L again (most of the time) and she is a fantastic teacher. She has only been a tech for 3 years, which helps because she remembers how overwhelming everything can be at first and how much there is to learn and how little time there is to learn it.In the in-patient dept they take care of all the other imaging exams that the out-patient dept doesnt. This includes all exams ordered for pts (patients) in the ED (Emergency Dept), those staying in the hospital, the maternity ward, and the OR. They do procedures that require fluoroscopy and the portable x-ray unit, and procedures that are more "invasive" like BEs, UGIs, esophograms and IVPs. Nuclear medicine, CT, MR and ultrasound are also assocated with this dept, however, specially trained techs do those procedures.
I'm finding out that it's all a very complex operation and there are about a million little details to get right for everything to turn out correctly. I have seen and learned a lot in the 2 short weeks I've been at clinicals, but I still have a long road ahead of me. I hope I can make it. Wish me luck.
Tuesday, August 29, 2006
I Survived My First Day of Clinicals!!!!
OK, sorry for the lack of posts the last few weeks, but I have been BIZZZZAYYY! Finals week drained me, but I survived. Then I had a week of vacation and my parents came into town for a few days and then all four of us (me, wife, mom and dad) drove out to San Francisco to visit my brother and his girlfriend. We had a great time and I will post some pics from our trip soon, I promise.
Then I got back and promptly returned to class, but luckily only on Monday. Then came today, my official first day of clinicals. Overall, it was a good day. I spent most of it getting oriented to the hospital, filling out paper work, meeting people in the dept and trying to find the cafeteria come lunch time. However, towards the end of the day I was able to assist another tech with x-raying two patients before the end of my shift came. Easy films, just a pelvis/hip and L-spine, but still a good first experience. The highlight was when one of the patients thanked me for helping her onto the table, the lowlight was when an old man coughed on the top of my head when I was helping to take off his pants. Oh well, I'll duck next time!
It's strange. I didnt really do much today in the way of seeing patients, but I'm still exhausted. Therefore, I don't have much to say right now. But stay tuned, I will do an update post this weekend and let you know how my first whole week at clinicals went. Wish me luck.
Then I got back and promptly returned to class, but luckily only on Monday. Then came today, my official first day of clinicals. Overall, it was a good day. I spent most of it getting oriented to the hospital, filling out paper work, meeting people in the dept and trying to find the cafeteria come lunch time. However, towards the end of the day I was able to assist another tech with x-raying two patients before the end of my shift came. Easy films, just a pelvis/hip and L-spine, but still a good first experience. The highlight was when one of the patients thanked me for helping her onto the table, the lowlight was when an old man coughed on the top of my head when I was helping to take off his pants. Oh well, I'll duck next time!
It's strange. I didnt really do much today in the way of seeing patients, but I'm still exhausted. Therefore, I don't have much to say right now. But stay tuned, I will do an update post this weekend and let you know how my first whole week at clinicals went. Wish me luck.
Monday, August 28, 2006
Wednesday, August 16, 2006
US lags
Ignorance is bliss.........for the ignorant. For the rest of us, it's just embarrassing.
Wow, one above Turkey. What an accomplishment. ugghhh!
Wow, one above Turkey. What an accomplishment. ugghhh!
Tuesday, August 15, 2006
Virtual Surgery
 Forget going to school for 12 years to become a doctor, who has the time?! Now YOU, yes YOU, can perform a complete knee replacement right in the comfort of your own home. Just click here to get started!
Forget going to school for 12 years to become a doctor, who has the time?! Now YOU, yes YOU, can perform a complete knee replacement right in the comfort of your own home. Just click here to get started!
Monday, August 14, 2006
Clinical Site Visit
I took a tour of my clinical site on Friday. It seems like a nice place. Not terribly huge but busy none the less. I also met my clinical instructor, who seems nice. It didn't fill me with complete confidence when I heard she has never had a student before and also just started working at this hospital a few months ago, but she seems to know her stuff and has been appointed as interim director of the dept until they can hire a full time director, so she must have a lot of experience under her belt.
Pros
- good shift: 8am-430pm Tu-F
- medium size hospital
- friendly staff in rad dept (seems to be so far, anyway)
- experienced clinical instructor
- meal vouchers for students (YES, free food!)
- I will be able to experience several modalities (CT, MR, Ultrasound, Nuc Med, etc.)
Cons
- they still use film, no CR or DR, ugh!
- it's a one hour drive (65 miles) from my house in Flag, which I will have to drive twice a day, 4 days a week for 8 months
- outpatient rad is separate from in-patient rad dept.
- clinical instructor has not had a student before
These are some of the apparent pros and cons of my site, but I'm sure I will find more when I start clinicals in a few weeks. Notice there are more pros than cons, and the cons that are there I can certainly live with.
In other news, this morning I took my first final exam of this semester. It was the written exam in my positioning class. I blasted through it and only had a few answers I wasn't 100% sure of. And thanks to the power of the interweb, I already know my grade and I got 100%, 0 wrong. Not too bad. But then again, I studied my butt off last week, so it's not like I didn't earn it. It's nice to have it over with though and even nicer to know I aced it! We have our lab competencies tomorrow for positioning, in which we get 3 positions at random (out of the over 60 we learned this semester) and have to demonstrate them for the instructor. I think I'm ready but just to make sure I plan to spend a few hours going over all of them at the coffee shop (the perfect study environment, at least for me) later today.
Pros
- good shift: 8am-430pm Tu-F
- medium size hospital
- friendly staff in rad dept (seems to be so far, anyway)
- experienced clinical instructor
- meal vouchers for students (YES, free food!)
- I will be able to experience several modalities (CT, MR, Ultrasound, Nuc Med, etc.)
Cons
- they still use film, no CR or DR, ugh!
- it's a one hour drive (65 miles) from my house in Flag, which I will have to drive twice a day, 4 days a week for 8 months
- outpatient rad is separate from in-patient rad dept.
- clinical instructor has not had a student before
These are some of the apparent pros and cons of my site, but I'm sure I will find more when I start clinicals in a few weeks. Notice there are more pros than cons, and the cons that are there I can certainly live with.
In other news, this morning I took my first final exam of this semester. It was the written exam in my positioning class. I blasted through it and only had a few answers I wasn't 100% sure of. And thanks to the power of the interweb, I already know my grade and I got 100%, 0 wrong. Not too bad. But then again, I studied my butt off last week, so it's not like I didn't earn it. It's nice to have it over with though and even nicer to know I aced it! We have our lab competencies tomorrow for positioning, in which we get 3 positions at random (out of the over 60 we learned this semester) and have to demonstrate them for the instructor. I think I'm ready but just to make sure I plan to spend a few hours going over all of them at the coffee shop (the perfect study environment, at least for me) later today.
Monday, August 07, 2006
ATV + 12 pack + 3am = Pain & Suffering
 Below is a quote from an email I got from my wife, a nurse on an orthopedic floor of the hospital:
Below is a quote from an email I got from my wife, a nurse on an orthopedic floor of the hospital:"Last night work kind of sucked. My patients were all nice, but I swear, the hallway I had was road rash alley. My patients were all males, between the ages of 27 and 39 and one was an ATV accident, 2 MVAs and the last guy was a bike vs. car, and he was the bike. He was hit from behind by a drunk driver going approx. 55 mph. Lucky to be alive. So they were all nice but my god, the dressing changes and pain medication, it just never ended. And just a fun fact: the ATV guy just had a birthday the previous night and decided to drink a 12-pack, get on his ATV at 3:00 in the morning, and of course crashed. Man, we were still picking pieces of glass and gravel out of him. Yuck. So just remember, DON'T drink your 12 pack and then ride your ATV, ok? I know it sounds crazy, but it isn't a good idea."
Thankfully she still has a sense of humor after seeing so much pain and injury. It never ceases to amaze me the patients she gets. They sure do make for interesting talk over dinner at the end of the day.
Sunday, August 06, 2006
X-ray images from Thulium
Here is an interesting video clip that was recently posted to a radiography forum. It was produced by the British Pathe Co. in the 1950's and talks about a battle-field "X-ray" unit, which uses a radioactive material called Thulium to make an x-ray image. The
image is formed on a Polaroid style film and presumably processed by the old
Polaroid camera method. Although called an "X-ray Unit" it actually uses Gamma rays to produce the image.
Here is an interesting video clip that was recently posted to a radiography forum. It was produced by the British Pathe Co. in the 1950's and talks about a battle-field "X-ray" unit, which uses a radioactive material called Thulium to make an x-ray image. The
image is formed on a Polaroid style film and presumably processed by the old
Polaroid camera method. Although called an "X-ray Unit" it actually uses Gamma rays to produce the image.
Thursday, August 03, 2006
Testsssssss
Phewwwww! This week has been a bit of a killer. 4 exams, 3 of which were on pretty hard material and lots of it. So I haven't had much of a chance to post. Apologies.
Otherwise, not much interesting has been happening, schoolwise anyway. Just biding my time and letting the semester burn itself out. Next week is a review week for all of our classes, since the following week is Finals Week. Yippeeee (insert sarcasm here). 6 major exams in 5 days. Strike that! in 4 days since I am opting to take my Friday exam early so I can get up to Flagstaff a day early. My parents are coming to town for a visit, so I need some extra time to clean the apt before they get there.
Unfortunately, my wife has been called to jury duty selection next week. She is really hoping to get out of it and has put in a call to her brother, who is a paralegal, for suggestions on how to disavow herself of this "honor". I know they say its your civic duty and you are doing a service for the community, yada, yada, yada. But it couldn't have come at a more inconvenient time with our trip to San Francisco planned in a couple of weeks. I also don't have much faith in the "jury of your peers" method the American legal system uses either. If, God forbid, I ever find myself in court, I don't feel real comfortable having my fate decided by Billy Bob the mechanic or Martha the diner waitress. But, hey, that's me. I'm really hoping she can get out of it. I'm thinking the fact that she is a nurse will help, but we'll just have to wait and see.
I realize this post isn't too radiography-related, but there hasnt been much developing on that front lately. At least not much that is post-worthy. So just boring personal stuff about yours truely will have to do for now. Thanks for your patience.
Otherwise, not much interesting has been happening, schoolwise anyway. Just biding my time and letting the semester burn itself out. Next week is a review week for all of our classes, since the following week is Finals Week. Yippeeee (insert sarcasm here). 6 major exams in 5 days. Strike that! in 4 days since I am opting to take my Friday exam early so I can get up to Flagstaff a day early. My parents are coming to town for a visit, so I need some extra time to clean the apt before they get there.
Unfortunately, my wife has been called to jury duty selection next week. She is really hoping to get out of it and has put in a call to her brother, who is a paralegal, for suggestions on how to disavow herself of this "honor". I know they say its your civic duty and you are doing a service for the community, yada, yada, yada. But it couldn't have come at a more inconvenient time with our trip to San Francisco planned in a couple of weeks. I also don't have much faith in the "jury of your peers" method the American legal system uses either. If, God forbid, I ever find myself in court, I don't feel real comfortable having my fate decided by Billy Bob the mechanic or Martha the diner waitress. But, hey, that's me. I'm really hoping she can get out of it. I'm thinking the fact that she is a nurse will help, but we'll just have to wait and see.
I realize this post isn't too radiography-related, but there hasnt been much developing on that front lately. At least not much that is post-worthy. So just boring personal stuff about yours truely will have to do for now. Thanks for your patience.
Thursday, July 27, 2006
How It Works - CT Scanners
 The next installment of my ongoing series called “How It Works” has to do with Computed Tomography, frequently referred to as CT imaging. Like conventional x-ray imaging, CT imaging uses x-rays to make images of the human body. However, CT imaging uses computers and a moving x-ray tube to obtain 3-dimenional, high-resolution, high-detail images of anatomical structures.
The next installment of my ongoing series called “How It Works” has to do with Computed Tomography, frequently referred to as CT imaging. Like conventional x-ray imaging, CT imaging uses x-rays to make images of the human body. However, CT imaging uses computers and a moving x-ray tube to obtain 3-dimenional, high-resolution, high-detail images of anatomical structures.History
The CT scanner was developed and demonstrated by Godfrey Hounsfield, a British physicist working for EMI, Ltd. Originally developing the idea in 1967, the first working prototype was unveiled in 1972. Atkinson Morley's Hospital in Wimbledon, England was the first institution to use a CT scanner to scan a patient. The first CT scanner sold in the US was to Massachusetts General Hospital and George Washington University for $390,000.
CT Technology
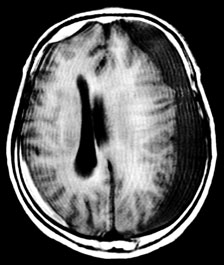
The first CT scanners were very limited in their applications compared to those used today. Primarily used to scan the brain, the earliest scanners could only form axial (horizontal) images of the human body; that is, a slice from side-to-side, similar to a slice of bread (see picture below). Thus the name Computed Axial Tomography, or CAT scan, was used to describe a scan from this machine. However, this name is no longer accurate, as today’s versions make it possible to see almost every structure in the body in a coronal, sagittal or axial plane, often in a clear 3-D view. Therefore, the term Computed Tomography, or CT imaging, has been adopted.

Axial, Coronal and Sagittal planes of the body
{kind=link}
CT - Axial View
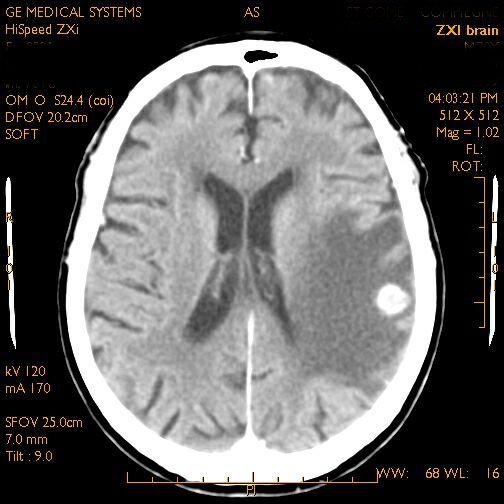
CT - Coronal View

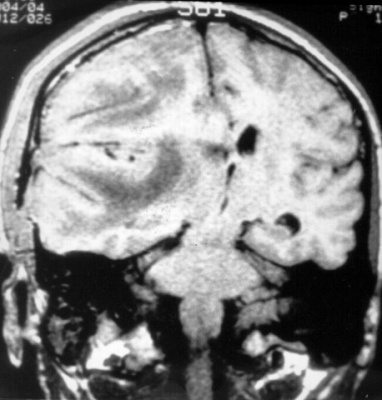
CT - Sagittal View
The CT scanner is a complex machine that relies on electronic/digital as well as mechanical equipment to make an image. The patient is placed on a movable platform that is raised and “inserted” into a short tube that looks something like a large donut. Within this tube is a revolving x-ray tube and image receptor (IR), or sensor. As the scan begins the x-ray tube begins to spiral around the patient emitting a thin curtain of x-rays as it moves. Directly across from the tube (on the other side of the patient) is a sensor that picks up the x-rays after they have passed through the patient, collects the data and transfers it to a computer. The computer then uses complex algorithms to form a visual image from the data and projects it onto a computer screen.
{kind=link}
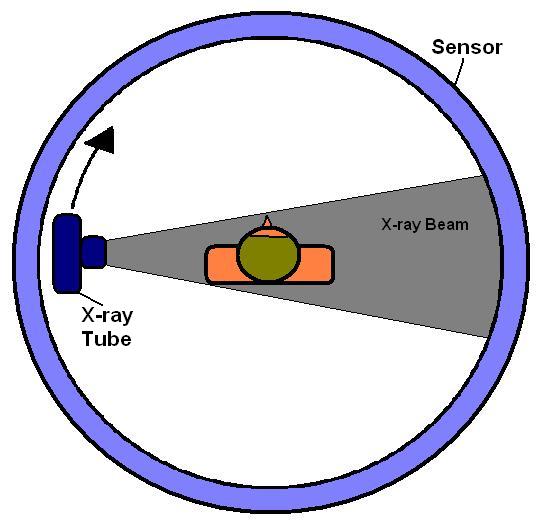
View of inner workings of a CT scanner; tube revolves around patient.
With conventional x-ray, different anatomical structures are superimposed on top of each other and often cannot be clearly seen on the x-ray image. However, with CT, because the x-ray tube and IR rotate around the patient’s body scanning it from all angles, it is able to combine all the data it receives from the scan into a comprehensible image for the doctor to evaluate. This is one of the reasons CT imaging is often considered “superior” to conventional x-ray imaging. However, there are some considerations to keep in mind.
A patient generally receives a higher dose of radiation when receiving a CT scan than a conventional x-ray. This is because the patient is being exposed to radiation during the entire time the CT is making its scan, which can last up to several minutes. However, with conventional x-ray the patient is exposed to just a brief emission of x-rays, often measured in just fractions of a second. This is why conventional x-ray is still used for simple imaging procedures such as a broken arm or finger or chest x-rays. Also, CT machines are not portable, so the patient must come to the machine, where as mobile x-ray units allow the machine to come to the patient’s room to make the image.
Conclusion
Overall, the computed tomography has proved to be an invaluable asset to medical imaging and has saved countless lives, whether from helping a doctor diagnose a brain tumor or allowing a surgeon to identify a brain bleed in a car accident victim. As technology advances it is likely that CT scanners will become faster, more precise and more compact, and will continue to allow medical professionals to save lives.
Grossness
 A quote from my positioning book in the Paranasal Sinuses chapter:
A quote from my positioning book in the Paranasal Sinuses chapter:"Exudate contained in the [paranasal] sinuses is not fluid in the usual sense of the word but is commonly a heavy, semigelatinous material. The exudate, rather than flowing freely, clings to the walls of the cavity and takes several minutes, depending on its viscosity, to shift position".
Eewwwwwwww!
Wednesday, July 26, 2006
Patient Obesity Is Obscuring Medical Scans
An article from Forbes online magazine. Here's the direct link to the article.
07.25.06, 12:00 AM ET
07.25.06, 12:00 AM ET
TUESDAY, July 25 (HealthDay News) -- In yet another example of how obesity is playing havoc with Americans' health, a new study finds that the number of inconclusive diagnostic imaging exams has doubled in the last 15 years -- a phenomenon experts attribute to all those extra pounds.
"Obesity is affecting the ability to image these people. We're having trouble finding out what's wrong," explained Dr. Raul N. Uppot, lead author of the study, and an assistant radiologist at Massachusetts General Hospital and an instructor in radiology at Harvard Medical School, both in Boston.
"When they come to the hospital, people are so concerned about the disease they have that they don't realize that being obese could hinder the ability to deliver health care," he said.
In fact, it could hinder it considerably, given medicine's ever-growing reliance on imaging technology such as X-rays and ultrasound.
"In the past 10 years or so, medicine has become so dependent on imaging," Uppot said. "Instead of doing very meticulous clinical examinations, a lot of doctors now rely on CT scans, ultrasounds, etcetera, to tell them what's happening inside the body. What happens when you're too big to fit on a table? Or you can fit on a table but the image is poor quality?"
The new study is published in the August issue of the journal Radiology.
The findings did not come as a surprise to outside experts. "The study shows more systemically what all of us felt was true anyway," said Dr. Levon Nazarian, professor of radiology and vice chairman for education at Thomas Jefferson University Hospital, in Philadelphia.
"Patients may not realize that there are two aspects to being overweight, one of which is the increased risk of a number of different diseases," Nazarian added. "They may not realize that once they actually get sick, their size is going to limit the ability to even tell them what's wrong."
According to official estimates, about two-thirds of adult Americans are overweight or obese, and the effect on individual health and the health-care system is considerable. Obese people are more likely to develop illnesses such as cancer, diabetes and heart disease. Hospitals have also had to "super-size" their wheelchairs and beds to accommodate the new generation of sick and overweight Americans.
To assess the effect of obesity on the quality of imaging exams, the researchers reviewed all radiology records from tests performed at Massachusetts General Hospital between 1989 and 2003. Specifically, they were looking at incomplete exams due to patient size.
"We looked at people who were able to fit on the imaging equipment and get the scan," Uppot said. "When radiologists read the film, they had trouble interpreting the film because the quality of the image was not very good because of [the patient's] size."
In 1989, 0.10 percent of inconclusive exams were due to patient size. By 2003, that number had almost doubled to 0.19 percent.
"What was most alarming was the increase," Uppot said. "The number itself was small."
Difficulties varied according to the type of imaging. By 2003, abdominal ultrasounds exhibited the most difficulty in giving a proper diagnosis (1.9 percent), followed by chest X-rays (0.18 percent), abdominal computed tomography (CT), abdominal X-rays, chest CT and magnetic resonance imaging (MRI).
Ultrasound sends high-frequency sound waves through the patient, where they bounce off internal organs and come back, like a submarine's sonar. But the thicker the fat, the less able the waves are to penetrate. A similar phenomenon is at work with X-rays, the study authors said.
CT scans and MRI have a different problem -- weight limitations of the table that holds the patient and the size of the opening on the imager.
"Many manufacturers have started to address the issue by increasing table weights," Uppot said.
The weight limit for CT scans has been increased from 450 pounds to 550 pounds. For MRI, the weight limit went from 350 to 550 pounds, he said.
But that doesn't solve the bigger problem. "We are now able to fit people on the machine. Then the issue is, what do you do?" Uppot said.
The imaging power can be increased on standard X-ray and CT machines, but this leads to an increase in radiation dose as well, he said.
"What we're realizing is that not only do obese people have increased health problems but our ability to deliver quality diagnostic imaging to them is limited," Uppot said. "A large patient can no longer walk into a hospital and say, 'I want the best quality care, let me get imaged and operated on.' If you're that big, there will be issues."
The problems don't stop with diagnosis. "It puts stress on personnel," said Dr. Jorge Guerra, professor of radiology at the University of Miami Miller School of Medicine. "X-ray personnel will be more prone to injury. We receive patients who are 400, 500, 600 pounds. It paralyzes our ability to provide care for other patients. We need special equipment, special beds, the imaging is lower quality so it takes longer to complete." Size also affects interventional radiology, or procedures meant to treat a patient, which is Guerra's specialty.
And as the University of Miami builds a new hospital, it is having to take into account that more than one-third of the patient population will be more than 350 pounds, he said.
Tuesday, July 18, 2006
Seasons
 Summer in Phoenix reminds me of winters growing up in Minnesota. "What!" you say "How can July in the sun-baked desert of Phoenix, Arizona remind you of the frozen, wind-blown tundra-like environment of Minnesota in January?" Well believe it or not it does.
Summer in Phoenix reminds me of winters growing up in Minnesota. "What!" you say "How can July in the sun-baked desert of Phoenix, Arizona remind you of the frozen, wind-blown tundra-like environment of Minnesota in January?" Well believe it or not it does.There are actually several similarities.
1. The weather is extreme: e.g. Minnesota in January = - 30 degress F, Arizona in July = 115 deg. F.
2. Everyone stays inside because it's either too hot or too cold to be outside for any length of time.
3. Energy usage hits an all time high for heating your homes in Minnesota and cooling them in Arizona.
4. Touching metal objects is a no-no and can result in either a nasty burn or painful frostbite.
5. Both cause me to question why anyone decided to settle here in the first place.
6. Nobody from out of state visits you.
7. You make trips to places with the opposite temperature: e.g. Mexico in the winter and Canada in the summer.
8. Plants and animals are doment and/or clinging to life.
9. Golf courses are suddenly empty.
10. You will refuse to go anywhere if the climate control is not working in your car.
So there you have it. Surprisingly there are several similarities between Minnesota winters and Arizona summers. Once you've experienced either one of them you are truely a survivor.
Monday, July 17, 2006
The poke heard 'round the world.......or at least in my apartment
 This weekend my wife was gracious enough to be my guinea pig for my very first attempt at venipuncture. What a doll!!
This weekend my wife was gracious enough to be my guinea pig for my very first attempt at venipuncture. What a doll!!I had called her early last week, and requested that she permanently "borrow" a butterfly needle or two from work, so I could practice venipuncture on her over the weekend. She obliged and on Sunday night at approximately 5:32 pm I inserted a metal needle into a person's vein for the very first time.
It wasn't without problems though. As a nurse, she has had plenty of experience putting in IVs and the like, so she walked me through the steps involved and before I knew it, it was my turn to try. I did all the prep, applied the tourniquet, cleaned the area with alcohol, located the vein and then dove in. He shoots and........he misses! Damn! Just as I slide the tip of the needle under the skin the bugger of a vein decides to do a little shimmy to the left, my right! With some soft cursing and the draining of what little confidence I had, I withdraw the needle and take a breath.
"It's OK," she tells me, "That happens a lot, just try to hold the skin tighter with your other hand so the vein can't move around." Infinite patience, this woman has. So I reprep, pick a different vein in the same hand and gear up again for insertion.
Holding the skin tighter so the vein has no where to go, I slip the needle under the skin in as smooth a motion as I can. It feels the same as before and I am just about ready to begin with the soft curses again, when I feel a light "pop" and a flash of blood appears in the clear tubing attached to the needle. I'm in!! Success!! I ask her how she's doing and she says "fine", although her face looks a little whiter than normal. I secure the butterfly portion of the needle with some tape, like we have to do for the comp test, and sit back and admire my work.
"Great job," she tells me, "now can you take it out, I'm not feeling so good." I glance up at her and her face is completely ashen. I quickly get to work removing the tape and then the needle. I tell her to put her head down between her knees, of which she is already in the process. She is a nurse after all. I have the needle out and am holding the gauze tightly against her hand when she sits back up and I can see some color returning to her face. "It's a lot easier when you are on the other end of the needle," she says, "now I know how my patients feel."
She's a little embarrassed about getting woozy, so I try to distract her with all my stupid stories about passing out at the doctors office when I was 16 after getting my first Hepatitis shot, and about going completely white and scaring the phlebotomists the first COUPLE of times I gave plasma. Within a few minutes she looks and feels better and tells me that her hand doesn't even hurt where I put in the needle. I take this as good news and explain to her that it's probably because of my unmatched, inherent skill at doing IV injections. She doesn't buy this for a second, but lets me believe it at least for a while.
A few hours later she suggests I try it one more time before I head back to Phoenix, just to make sure I have the process down. Once again I do all the prep. I take her other hand this time and insert the needle and get flashback right away. Success again. This time she doesn't watch or talk during it and just lets me do it all myself. I think this helps, because this time she doesn't get woozy at all and says that she only felt a slight pinch right when I put in the needle, but after that no pain. I guess my practice is paying off.
What a sweetheart letting me practice venipuncture on her. However, she has already told me that when it comes time to test off on administering Barium enemas, I will have to find myself someone else to practice on. Can you blame her?
Favorite Photos
Check out some of my favorite photos that my wife and I have taken. What do you think? Maybe a new hobby?!
Wednesday, July 12, 2006
Radiologic Technologist, X-ray Tech, Rad Tech, Radiographer, Medical Imaging
 If you are considering a career as a Radiologic Technologist (aka X-ray Tech), have I got a page for you. Please check out Desert Imaging II: A Blog for Prospective X-ray Technologist Students. It provides some basic and not so basic information about the job of Radiologic Technologist.
If you are considering a career as a Radiologic Technologist (aka X-ray Tech), have I got a page for you. Please check out Desert Imaging II: A Blog for Prospective X-ray Technologist Students. It provides some basic and not so basic information about the job of Radiologic Technologist.In the blog, I talk about the educational background you will need as well as things to expect when you start the job. Also, there are many useful links to webpages with additional information on medical imaging.
Please take a moment to check it out if you are interested in becoming a Radiologic Technologist.
Tuesday, July 11, 2006
T is for Technologist
TECHNOLOGIST v. TECHNICIAN. What's the difference, you ask? In radiography circles, the difference is huge!
For many years the term X-ray Technician, or radiology technician, was used to describe the healthcare worker who was in charge of creating x-ray images of sick or hurt patients. They had little, or no, formal education, were trained on the job and were not licensed or credentialed in any way.
That has all changed. Although still misused by the lay-person, and even some people within the healthcare field, x-ray technician is no longer an accurate title for the personnel who are involved in creating medical images.
Currently, we are in a period of transition. Although the term technician is no longer used, a solid, universally-accepted title has not yet been estabished. I guess the most commonly used title in the US, and one endorsed by our major certifying organization the ARRT, is Radiologic Technologist. The title is right there in their name (American Registry of Radiologic Technologists). After taking a nationally recognized exam administered by the ARRT, a student becomes certified as a Technologist, is registered with the ARRT, and can later take another exam to be licensed in the state in which the tech works.
However, that's not to say other names are not used in everyday conversation. X-ray Technologist is still common, as is Rad Tech and RT. Radiographer is commonly used in Great Britain and is likely derived from our common use of the word photographer (a person who make pictures with light rather than x-ray radition). Imaging Tech is more general, including techs who work in CT, MR and ultrasound, and more accurate in that these modalities all produce images of the human body, but they do not all use x-ray radiation to do it.
Presently, radiology departments are employing a level of imaging worker that is similar to the antiquated X-ray Technician, called a Practical Technologist or X-ray Tech of limited scope. This position requires less education than an Radiologic Technologist and is much more limited in their scope of practice, as the name would imply. They are certified to image parts of the distal extremeties, the shoulder girdle, the chest, skull and spine. They are NOT able to image the GI tract, the pelvis, the reproductive tract, the urinary tract or work in Specials. Also, they can NOT use fluoroscopy, CT, MR or bone densitometry. And because of their limited capacity this position is being phased out in many of the hospitals around the United States.
Still a little confused? One way to look at it is comparing a Radiologic Technologist to a Technician is like comparing an RN with an LPN or a physician with a physician's assistant. While all positions in healthcare are important and worthy of respect (right down to the guy who mops the floors), there are often vast differences in education, experience and scope of practice between the different branches in the healthcare hierarchy.
Another way to look at it (and I can't take credit for this, since it's something my instructor told us) is that:
For many years the term X-ray Technician, or radiology technician, was used to describe the healthcare worker who was in charge of creating x-ray images of sick or hurt patients. They had little, or no, formal education, were trained on the job and were not licensed or credentialed in any way.
That has all changed. Although still misused by the lay-person, and even some people within the healthcare field, x-ray technician is no longer an accurate title for the personnel who are involved in creating medical images.
Currently, we are in a period of transition. Although the term technician is no longer used, a solid, universally-accepted title has not yet been estabished. I guess the most commonly used title in the US, and one endorsed by our major certifying organization the ARRT, is Radiologic Technologist. The title is right there in their name (American Registry of Radiologic Technologists). After taking a nationally recognized exam administered by the ARRT, a student becomes certified as a Technologist, is registered with the ARRT, and can later take another exam to be licensed in the state in which the tech works.
However, that's not to say other names are not used in everyday conversation. X-ray Technologist is still common, as is Rad Tech and RT. Radiographer is commonly used in Great Britain and is likely derived from our common use of the word photographer (a person who make pictures with light rather than x-ray radition). Imaging Tech is more general, including techs who work in CT, MR and ultrasound, and more accurate in that these modalities all produce images of the human body, but they do not all use x-ray radiation to do it.
Presently, radiology departments are employing a level of imaging worker that is similar to the antiquated X-ray Technician, called a Practical Technologist or X-ray Tech of limited scope. This position requires less education than an Radiologic Technologist and is much more limited in their scope of practice, as the name would imply. They are certified to image parts of the distal extremeties, the shoulder girdle, the chest, skull and spine. They are NOT able to image the GI tract, the pelvis, the reproductive tract, the urinary tract or work in Specials. Also, they can NOT use fluoroscopy, CT, MR or bone densitometry. And because of their limited capacity this position is being phased out in many of the hospitals around the United States.
Still a little confused? One way to look at it is comparing a Radiologic Technologist to a Technician is like comparing an RN with an LPN or a physician with a physician's assistant. While all positions in healthcare are important and worthy of respect (right down to the guy who mops the floors), there are often vast differences in education, experience and scope of practice between the different branches in the healthcare hierarchy.
Another way to look at it (and I can't take credit for this, since it's something my instructor told us) is that:
A Technician is TRAINED
A Technologist is EDUCATED
or
A Technologist is EDUCATED
or
A Technician can push the button
and a Technologist knows why.
and a Technologist knows why.
I hope this information has helped clear up the difference between a technician and a technologist. Keep in mind terminology and practices differ from region to region and between institutions, so this information may not be entirely accurate in all instances. But in a general way it should help you to realize that a difference exists between the two terms and it is important to use the correct one when referring to a Radiologic Technologist.
Factoid #1548
 If properly motivated, I can eat an entire box of Krispy Kreame donuts and still resect myself in the morning.
If properly motivated, I can eat an entire box of Krispy Kreame donuts and still resect myself in the morning.
Monday, July 10, 2006
3-D gaming tech used to train Radiographers
Here's a link to a BBC News article on how 3-D gaming technology is being employeed to train student radiographers on patient positioning and other aspects of radiography. Check it out!
Friday, July 07, 2006
Update
Re: the "Hardest Test EVER" test
Well, I guess it wasn't so hard after all since I apparently got 99%. Don't ask me how though. :-)
Well, I guess it wasn't so hard after all since I apparently got 99%. Don't ask me how though. :-)
Thursday, July 06, 2006
Hardest test.....EVER!!!
OK, maybe not the hardest test EVER, but pretty hard anyway. It was one of the most difficult tests so far in my radiography program. It was in Radiographic Techniques, and although I think I did pretty well, I left the classroom brain-fried.
It was one of those tests with questions like:
"If you increase focal spot size how does it affect image detail?", "If kVP is increased by 15% what will happen to image density?", "When you increase OID what happens to radiographic contrast?" "If the patient is larger than average how will the increase in patient thickness affect image density and detail?" yada, yada, yada, blah, blah, blah, etc., etc., etc.......
A lot of if-then statements.........YUCK!! There seem to be endless variables you can change when making an image of a patient, and we have to know what will happen to the image if one or more of those variables are changed. It's a lot to keep straight in your head without having any experience in making x-ray images to use as a reference.
Our instructors said it will come together during clinicals (we shall see!), but for now we essentially had to memorize a + and - chart which tells us how one variable is affected if another variable is increased or decreased. For example, if you increase the mAs (which stands for milliamperes per second) you are basically increasing the amount of radiation leaving the x-ray tube. This increase in radiation means that more radiation will penetrate the patient and pass through to the other side, which in turn exposes more of the x-ray film making it appear more dark or have a higher visual density (degree of blackness).
Here's the chart, in case you're curious.
 + = increase, - = decrease, O = no change
+ = increase, - = decrease, O = no change
Fun stuff, huh!?
It was one of those tests with questions like:
"If you increase focal spot size how does it affect image detail?", "If kVP is increased by 15% what will happen to image density?", "When you increase OID what happens to radiographic contrast?" "If the patient is larger than average how will the increase in patient thickness affect image density and detail?" yada, yada, yada, blah, blah, blah, etc., etc., etc.......
A lot of if-then statements.........YUCK!! There seem to be endless variables you can change when making an image of a patient, and we have to know what will happen to the image if one or more of those variables are changed. It's a lot to keep straight in your head without having any experience in making x-ray images to use as a reference.
Our instructors said it will come together during clinicals (we shall see!), but for now we essentially had to memorize a + and - chart which tells us how one variable is affected if another variable is increased or decreased. For example, if you increase the mAs (which stands for milliamperes per second) you are basically increasing the amount of radiation leaving the x-ray tube. This increase in radiation means that more radiation will penetrate the patient and pass through to the other side, which in turn exposes more of the x-ray film making it appear more dark or have a higher visual density (degree of blackness).
Here's the chart, in case you're curious.
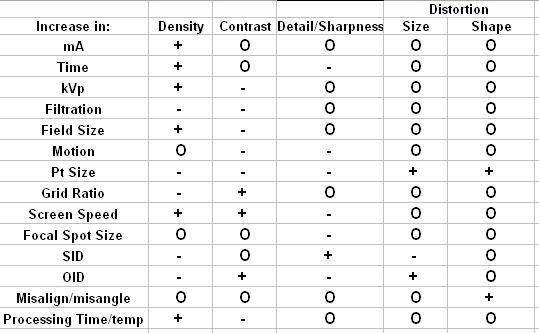 + = increase, - = decrease, O = no change
+ = increase, - = decrease, O = no changeFun stuff, huh!?
Thursday, June 29, 2006
Pigg-o-stat
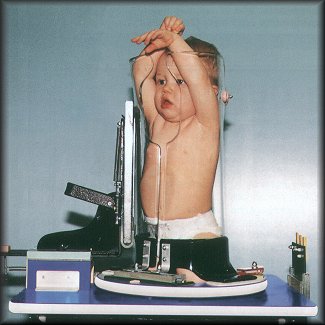 Well folks, meet the Pigg-o-stat. Also known by its more PC name, the Pediatric Immobilizer and Positioner. Although it looks like some kind of Medevil torture device, it's actually used to "immobilize" squirmy, wiggly little ones while we attempt to get a chest x-ray of them.
Well folks, meet the Pigg-o-stat. Also known by its more PC name, the Pediatric Immobilizer and Positioner. Although it looks like some kind of Medevil torture device, it's actually used to "immobilize" squirmy, wiggly little ones while we attempt to get a chest x-ray of them.It's interesting to note the look on the kid's face in the pictures. I assure you they don't often look like that in real life. Most of the time they are screaming their little lungs out (which, consequently makes for a better chest x-ray) with snot running down their face.
 Luckily, the whole procedure takes about as much time as it takes you to tie your shoes, but that doesn't mean the first sight of the thing doesn't scare the hell out of the kid, or the parents for that matter. For obvious reasons it's only used as a last resort, after all attempts to manually immobilize the child have been exhausted. Also, the children it is used for are often so small/young, they wont remember the whole traumatic experience and soon after being liberated from the dreaded apparatus are back to happily sticking legos up their noses as toddlers have done for centuries.....well, decades anyway.
Luckily, the whole procedure takes about as much time as it takes you to tie your shoes, but that doesn't mean the first sight of the thing doesn't scare the hell out of the kid, or the parents for that matter. For obvious reasons it's only used as a last resort, after all attempts to manually immobilize the child have been exhausted. Also, the children it is used for are often so small/young, they wont remember the whole traumatic experience and soon after being liberated from the dreaded apparatus are back to happily sticking legos up their noses as toddlers have done for centuries.....well, decades anyway.Usually, the parents are asked to don lead shield aprons and sit with the children for reassurance during the exam, but ultimately it rests on the radiographer to make the patient as comfortable and non-traumatized as possible. I am not looking forward to the first time I have to put an itty-bitty patient in one of these contraptions. Let the screaming commence.
Monday, June 26, 2006
VVMC
Verde Valley Medical Center. That's the name of the site for my first clinical rotation!!! VVMC is in Cottonwood, Arizona, a sleepy little desert town of about 10,000 people located in the high desert of central Arizona. Although the city itself is small, the hospital services much of the rural population of central Arizona.
 View from Tuzigoot Monument near Cottonwood, AZ
View from Tuzigoot Monument near Cottonwood, AZ
I can't believe how everything played out. As I have explained before, the way the draw worked is that the names of everyone in my Outer Site group (i.e. sites not located in the Phoenix metro area) were put into a bowl and our instructor pulled the names one-by-one at random. As each name was pulled that person got to choose which clinical site they wanted from a predetermined list of hospitals and clinics that our instructors gave us. As luck would have it, I was the FIRST name pulled. Can you believe that!!! I never have that kind of luck.
Unfortunately, the day before I had found out that Flagstaff Medical Center was not accepting students this semester, so I had decided my second choice was Verde Valley Medical Center in Cottonwood. So of course I jumped on VVMC and am now officially assigned to that site. Cottonwood is about 65 miles or an hour's drive from my apartment in Flagstaff. So, althoug it means a lot of driving, I will be able to live at home in Flagstaff with Becky and Imara again. Yay!!!
In a few weeks, I will be contacted by my clinical instructor and will have to visit the hospital for an orientation meeting. I can't wait to get started. I wish I didnt have to wait until mid-August for clinicals to start. :-(
I apologize for keeping you all hanging regarding which site I got. Its just that I was sick for a few days after the draw and spent most of the time in bed, then we drove out to Santa Fe, NM this weekend for a friend's wedding, and I just got back last night. Santa Fe is a beautiful city and I hope to post some pics soon. Stay tuned. :-)
 View from Tuzigoot Monument near Cottonwood, AZ
View from Tuzigoot Monument near Cottonwood, AZI can't believe how everything played out. As I have explained before, the way the draw worked is that the names of everyone in my Outer Site group (i.e. sites not located in the Phoenix metro area) were put into a bowl and our instructor pulled the names one-by-one at random. As each name was pulled that person got to choose which clinical site they wanted from a predetermined list of hospitals and clinics that our instructors gave us. As luck would have it, I was the FIRST name pulled. Can you believe that!!! I never have that kind of luck.
Unfortunately, the day before I had found out that Flagstaff Medical Center was not accepting students this semester, so I had decided my second choice was Verde Valley Medical Center in Cottonwood. So of course I jumped on VVMC and am now officially assigned to that site. Cottonwood is about 65 miles or an hour's drive from my apartment in Flagstaff. So, althoug it means a lot of driving, I will be able to live at home in Flagstaff with Becky and Imara again. Yay!!!
In a few weeks, I will be contacted by my clinical instructor and will have to visit the hospital for an orientation meeting. I can't wait to get started. I wish I didnt have to wait until mid-August for clinicals to start. :-(
I apologize for keeping you all hanging regarding which site I got. Its just that I was sick for a few days after the draw and spent most of the time in bed, then we drove out to Santa Fe, NM this weekend for a friend's wedding, and I just got back last night. Santa Fe is a beautiful city and I hope to post some pics soon. Stay tuned. :-)
Monday, June 19, 2006
Clinical Site
 Most people look forward to the end of the day. They long to flop into bed, ready to say hi to Mr. Sandman. I do too. Or at least I did until last week. I havent slept more than a few hours each night for the last several days. I lay my pretty little head down at night and sit and stew. I worry about where I will end up for my first clinical rotation.
Most people look forward to the end of the day. They long to flop into bed, ready to say hi to Mr. Sandman. I do too. Or at least I did until last week. I havent slept more than a few hours each night for the last several days. I lay my pretty little head down at night and sit and stew. I worry about where I will end up for my first clinical rotation.I just found out today that Flagstaff is not accepting students this semester for clinicals, so that choice is off the board. My next choice is a hospital in the small town of Cottonwood, AZ, which is about 65 miles from Flagstaff, just close enough for me to live at home in Flagstaff again and drive each day to clinicals. Sure it means a lot of driving, but if it also means I get to live at home with my wife and cat, not pay two rents each month and have one food bill, then so be it.
Unfortunately, I am not assured this site. The way our system works is that everyone's name is put into a bowl and our instructor pulls the names from the hat one by one and that is the order in which we get to choose our site. A so-called "random" drawing. Not so random for me since I have just about the worst luck with this kind of thing as any human on earth living or dead.
Anyway, I'm in competition with at least 10 other people who want the same site as me. Granted I have 2nd, 3rd, 4th, 5th, and 6th choices, but I would rather not fall back onto those, as they would entail endless driving, double rents, and a prolonged absence from my family (family = Becky plus cat), who I have grown quite fawned of as of late.
For these reasons, I have found it difficult, if not impossible, to get to sleep and stay that way for the last week or so. I know its silly because there is nothing I can change until the day we draw, which is tomorrow by the way, but still my little brain gets to working, and worrying, and I run over all the scenarios in mind until I'm so worked up sleep is not even on my radar anymore.
At least by lunch time tomorrow it will all be over one way or another. I just hope my historically bad luck takes a turn for the better and I get the site I want. I really need some stability right now, and actually living at home again would really provide that for me.
So if you happen to see a falling star tonight, please keep me in mind when you do your wishing. I will probably be up all night anyway, and I plan to do a lot of wishing of my own.
Word of the Day
 Defecography!!!
Defecography!!!Defecography is a functional study of the distal colon, which includes fluoroscopic or radiographic imaging during defecation and is used to evaluate fecal incontinence and other functional problems of the lower GI.
If you can't tell, this chapter in positioning has to do with imaging the upper and lower GI (Gastrointestinal) system and there are several new procedures we have to learn, one of them being defecography.
Defecography is not an uncommon procedure and it can be performed at most hospitals and imaging clinics. However, in my opinion, the way they go about getting the images is a bit.....ummm odd.
In order to visualize soft tissue (e.g. parts of the digestive tract), a contrast material must be used. A contrast material, often just called contrast, is a substance that is radio-opaque, or does not allow x-rays to pass through it, and shows up as white on the radiograph (aka x-ray image). The contrast material most often used for contrast studies of the GI system is barium sulfate. Barium usually comes in liquid or semi-liquid form and generally has the consistency of pepto bismol, so that it coats the walls of your GI tract and also does not pass through too quickly. It's administered either orally or via a barium enema.
Defecographs are different in that they are a functional study and the actual movement of the colon is observed using fluoroscopy, a sort of live, moving x-ray. But for the colon to be able to act on the barium contrast in order for the radiologist to observe function, the contrast must have a thicker consistency than a pepto bismol-like liquid.
Here is where it gets interesting. A common practice among radiographers is to mix the regular barium liquid with freeze-dried instant potato flakes in order to obtain the proper consistency. Of course, other substances have been tried, but most don't offer the proper consistency, even dispersion of barium and "cost effectiveness" as simple, over-the-counter instant potatoes.
So if you ever have the need for a defecography study, just know that somewhere in Idaho a farmer worked very hard on his harvest just so the doctor could get a good look at your large intestine in action.
Subscribe to:
Comments (Atom)